
Condensing the referral-to-first fraction workflow
Radiation Oncology Solutions
User experiences
The South West Wales Cancer Centre reimagines complex radiotherapy workflows
The South West Wales Cancer Centre (SWWCC, Swansea Bay University Health Board, UK) is working with Philips to address the issues surrounding complicated radiotherapy (RT) workflows, a strategy aimed at simplifying and accelerating the patient’s path from referral to treatment. SWWCC is among the first partner sites that will implement Philips’ IntelliSpace for Radiation Oncology and associated practice management solutions.
“The risk of local recurrence grows with increasing radiotherapy waiting times and this results in decreased survival in some clinical situations”

Dr. Russell Banner
Dr. Russell Banner has been a consultant clinical oncologist in the South West Wales Cancer Centre since 2013. His specialist tumour sites are head and neck, gynaecological and skin cancers. He is active as Principal Investigator for a number of UK-wide clinical research radiotherapy trials and has a deep interest in radiotherapy quality improvements in his role as radiotherapy lead.
Complex radiotherapy workflows
Staff at radiation oncology departments worldwide are well familiar with the necessary, but painstaking, fragmented and labor-intensive process of navigating the radiotherapy treatment process from patient referral to first fraction. The path from simulation to a workable plan remains a mostly manual process with frequent handovers, waiting times and lags in data transfers between systems. The path entails hundreds of mouse clicks, logging in and out of disparate information systems and an over-reliance on human interaction and communication to ensure quality and certainty along the way. SWWCC is addressing the complexity of this process. In their co-creation partnership with Philips (see sidebar), SWWCC is involved in the development of both Philips’ IntelliSpace Radiation Oncology patient management solution (see sidebar) and the allied services that are part of the company’s Radiation Oncology Practice Management.
What is IntelliSpace Radiation Oncology?
IntelliSpace Radiation Oncology is an intelligent patient management solution designed to accelerate the time from patient referral to the start of treatment. With a protocol-driven care pathway the radiotherapy workflow, departmental efficiency as well as operational excellence can be improved. A key principle underlying IntelliSpace Radiation Oncology is to start with the physician’s intent for the patient, as it will trigger many subsequent steps in the workflow. It is also designed to be vendor-neutral, so a department can interface with many of their third-party solutions, whether it is a treatment planning system or a contouring tool.
Radiation Oncology Practice Management is a partnership solution offering a flexible suite of services, tools, and support to help enable optimal use of resources for effective patient-centric care. Philips collaborates with each center to customize IntelliSpace Radiation Oncology to meet specific departmental requirements and workflows and tailors training to assure staff proficiency.
Patients also demand shorter waiting times”
Decreasing time to radiotherapy is important
“Reducing the time to the patient’s first fraction is important, Dr. Banner says. “The negative clinical impact of delaying patient treatment isn’t just theory anymore, there is an evidence base now. The risk of local recurrence grows with increasing radiotherapy waiting times and this results in decreased survival in some clinical situations.1-3 “Patients also demand shorter waiting times,” he adds. “In Quebec a class-action was brought to court on behalf of patients who were waiting too long for their radiotherapy treatment on the basis it would increase local recurrence rates.”4
“When I started in 2013, I concentrated first on decreasing the time to RT for adjuvant head-and- neck patients to boost overall survival. Delays were far too long with an average time to treatment of 12 weeks and high variation (see figure 1), Dr. Banner says. “We reduced the wait times initially by speaking with our surgeons and stressing the importance of working together, but we also focused on ways to condense the radiotherapy planning workflow. We implemented new ways of workings, such as using checklists and remove approval of plans in MOSAIQ, moving from paper booking to electronic booking and migrating all of our systems onto the Citrix platform to facilitate remote access. Performance continues to improve on this small group of about two patients each week, so that now over 75 percent of patients start within six weeks of surgery. But variability remains, and we want to make similar improvements for all patients having radiotherapy.”
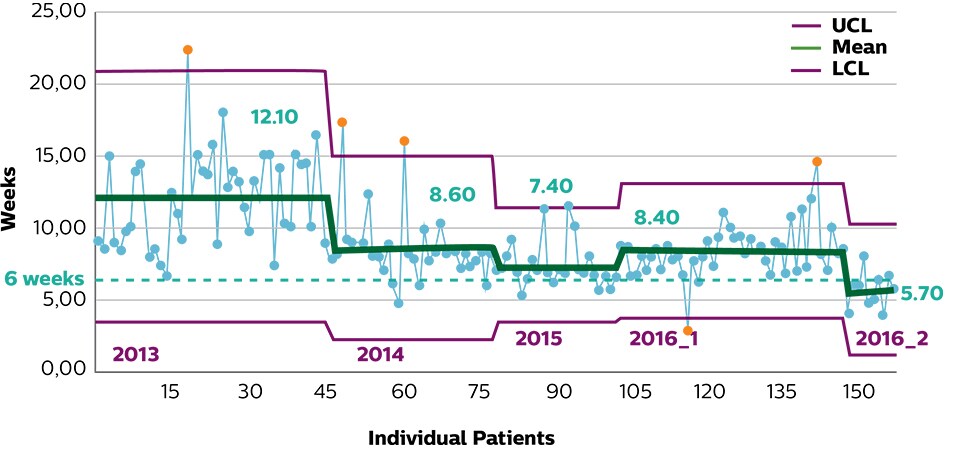
Figure 1. Average time between surgery and radiotherapy by date of surgery for locally advanced head-and-neck patients.
Critical impact of protocol compliance
“Besides excessively long wait times, we know that protocol deviations impact local control5,” Dr. Banner says. “We also know that in clinical trials, we have great radiotherapy quality assurance,” he continues. “How do we inject that level of quality assurance into our day-to-day clinical practice for all of our patients? We know it is important, but the radiotherapy process is complex. From referral, through imaging, image registration, all the way through to the first fraction.” “Getting things done quickly is not the only important focus. Getting them done right means following the protocol”.
Partnering with automation to address increase in workload
With limited human and treatment resources (see SWWCC Facts), the radiotherapy department of SWWCC is not unlike many UK cancer clinics, Dr. Banner observes. “I recently saw an interesting comment on my Twitter feed,” he says. “The tweet was complaining about the multiple passwords and PINs in daily oncology practice in the 2019 NHS environment. It causes a great deal of frustration.”
“Our workforce is stretched and could be bigger, especially since we’re expecting an increase in our workload,” he says. “We already brought down our time to radiotherapy, but in our view it is still not good enough. We have an excellent team with RTTs, physicists, dosimetrists and clinicians working together. We all know what we want to achieve, but we have limited resources. We see the opportunity to go so much further with automation and better interoperability of our systems.”
SWWCC’s experience is a mirror image of many radiation therapy departments throughout the UK; the number and complexity of the different systems departments use compound the problem.
Figure 2. Reported example from Twitter of up to 16 different passwords/PINs needed for day-to-day oncology practice in 2019.
Figure 1. Reported example from Twitter of up to 16 different passwords/PINs needed for day-to-day oncology practice in 2019.
SWWCC to be first “laboratory” for developing IntelliSpace Radiation Oncology and Practice Management
“In our practice we see that there are many uncertainties along the way, a lot of hand-overs and waiting time. That impacts on quality and patient throughput,” Dr. Banner says. “We know that adding workflow automation and optimizing the radiotherapy process will help. This is why we teamed up with Philips”.
“Working with Philips, we see the opportunity to go so much further with automation and streamlining our processes,” he continues. “It can improve the consistency of care using a protocol-driven workflow and enhance care quality by integrating applications we employ into the pathway seamlessly. We want it all to be smoother so we can reduce the time to the first fraction. We can do this by improving communication between teams and purposely redesigning workflows with specialists.”
Working with Philips we see the opportunity to go so much further with automation”
Understanding the entire workflow is key
“Being protocol-driven, it is pointless to integrate a patient management solution like IntelliSpace Radiation Oncology without appreciating what the whole pathway looks like,” Dr. Banner says. Working with Philips consultants, SWWCC chose to initially map its breast radiotherapy pathway, convening a mapping workshop that involved the entire multi-disciplinary team, including administrative staff, radiation oncologists, physicists, dosimetrists and radiation therapy technologists. See figure 4 for the current Swansea Breast Pathway.
As a preparatory phase before implementing actual solutions, SWWCC worked to gain an in depth understanding of each radiotherapy workflow – where it is efficient and where the bottlenecks are.
“We found out quite a lot,” Dr. Banner says. “We think we know what tasks everyone does in the workflow, but we’re checking and re-checking things constantly – sometimes we check critical things seven times. It is a matter of safety. But how many times do we really need to check that particular part of the workflow?”

Figure 3. SWWCC Breast pathway mapping workshop.
Figure 2. SWWCC Breast pathway mapping workshop.
14-step Breast Pathway
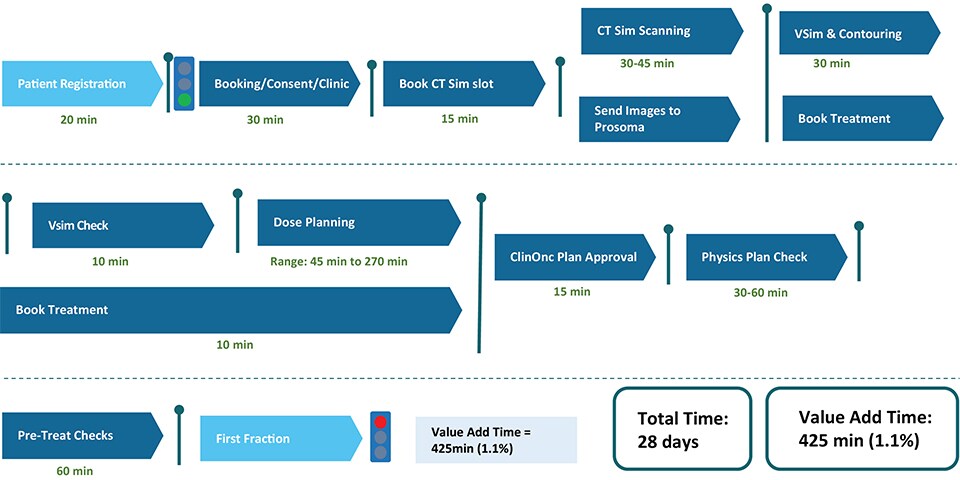
Figure 4. Current breast pathway at SWWCC.
In addition to decreasing the patients’ time to treatment, patients will also benefit by helping us as clinicians to consistently treat every patient to the highest quality levels”
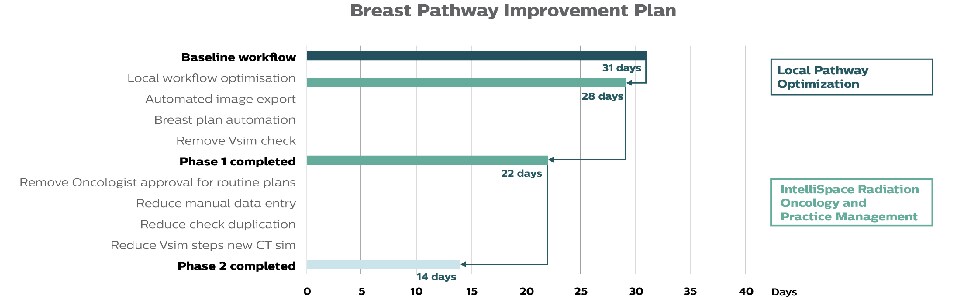
Figure 5. Referral to first treatment times at SWWCC.
Condensing the referral-to-first fraction interval from 28 days to 14 days for breast cancer patients
“Our breast pathway has 14 high-level workflow steps in it,” Dr. Banner says. “Our previous local workflow optimization activities had brought the referral-to-first treatment interval down from 32 to 28 days. Collaborating with the Philips consultants we aim to get the interval down from 28 to 22 days and that is what we’re implementing for the breast radiotherapy pathway now,” he notes. “With additional workflow improvements and full implementation of IntelliSpace Radiation Oncology we think it is realistic and achievable to bring the referral-to-first fraction period down to just 14 days.
Benefits for both caregivers and patients
“We know that Philips’ workflow innovations are going to be really helpful. The IntelliSpace Radiation Oncology automation alone is going to be brilliant,” Dr. Banner says. “But technology isn’t the only answer. We are experiencing that the combination with Practice Management consultancy can truly streamline the radiotherapy workflow and allow us to improve clinical outcomes. In addition to decreasing the patients’ time to treatment, patients will also benefit by helping us as clinicians to consistently treat every patient to the highest quality levels, aiming to replicate the benefits we see when we treat patients in protocolized clinical trials. It should help us sit down to plan patients at the right time, in the right electronic space. Finally, IntelliSpace Radiation Oncology will allow us to manage our workflows within our department, seeing where patients are within the often complex treatment pathways.”
References
1. Chen Z, King W, Pearcy R, Mackillop WJ. The relationship between waiting time for radiotherapy and clinical outcomes: a systematic review. Radiother Oncol. 2008 Apr;87(1):3-16. 2. Ang KK, Trotti A, Brown BW, et al. Randomized trial addressing risk features and time factors of surgery plus radiotherapy in advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2001 Nov 1;51(3):571-8. 3. Cattaneo R II, Hanna RK, Jacobsen G, Elshaikh MA. Interval between hysterectomy and start of radiation treatment is predictive of recurrence in patients with endometrial carcinoma. Int J Radiat Oncol Biol Phys. 2014 Mar 15;88(4):866-71. 4. Gupta S, King WD, Korzeniowski M, Wallace DL, Mackillop WJ. The effect of waiting times for postoperative radiotherapy on outcomes for women receiving partial mastectomy for breast cancer: a systematic review and meta-analysis. Clin Oncol (R Coll Radiol) 2016 Dec; 28(12):739-749. 5. Wuthrick EJ, Zhang Q et al. 2015. Institutional Clinical Trial Accrual Volume and Survival of Patients With Head and Neck Cancer. Journal of Clinical Oncology 33:156-164.
Results are specific to the institution where they were obtained and may not reflect the results achievable at other institutions.